
The best treatment is prevention.
Get ahead of injuries…not behind them.
Injury prevention in throwing sports is a shared responsibility across athletes, coaches, parents, and clinicians. The forces involved in overhead throwing are significant, and the cumulative demands of a long season push the limits of what the body can repeatedly tolerate. With the right awareness, load management, and early intervention, many of these injuries are preventable. This page synthesizes the current evidence into practical guidance for everyone in the circle of care around a throwing athlete.
Injury Prevention for Throwers
Throwing is one of the most physically demanding actions the human body performs. The forces generated at the elbow and shoulder during a single pitch are remarkable: during the acceleration phase, the shoulder internally rotates at peak angular velocities approaching 7,000–7,500 degrees per second, making it one of the fastest known human motions. When repeated hundreds or thousands of times across a season, the cumulative load on developing and adult throwers is significant.
Injury rates in baseball and softball have been climbing for years, particularly among younger athletes. While some degree of risk is inherent to the sport, many of these injuries are preventable. With appropriate load management, early awareness, and timely intervention, we can help reduce these numbers. Early recognition and intervention are key.
And that’s what this page is about.
Understanding Throwing Injuries
The throwing motion is one of the fastest and most violent movements in all of sport. The acceleration phase, from maximum external rotation to ball release, occurs in approximately 50 milliseconds. In that fraction of a second, the shoulder and elbow are subjected to forces that push the limits of what soft tissue and bone can repeatedly tolerate.
This matters because throwing isn’t a single high-effort event; it’s a repetitive one. A starting pitcher may throw 80–100 pitches in a game. A catcher throws down to second dozens of times in a practice. A little leaguer may play on two or three teams simultaneously across an extended season. That cumulative load, more than any single throw, is what ultimately drives injury.
In fact, most throwing injuries aren’t the result of one bad throw. They develop gradually through accumulated stress, insufficient recovery, or physical deficits that quietly compound over time. By the time pain becomes noticeable, the underlying issue is often well established. This is precisely why awareness and early action matter.
Needing some guidance on arm care?
We’ve put together one of the most comprehensive injury prevention resources available for throwing athletes. Drawing from over a dozen peer-reviewed studies and established guidelines, it covers everything from key risk factors and workload management to audience-specific prevention strategies for athletes, coaches, parents, and clinicians. Download it, share it, and put it to use.



Key Risk Factors
Understanding why throwing injuries happen is the first step toward preventing them. The research points to several consistent, well-established risk factors, most of which are modifiable with the right awareness and habits
1. Workload & Volume
- The single most studied risk factor in throwing athletes. Higher pitch counts, more innings pitched, and longer seasons are each independently associated with increased injury risk.
- Exceeding recommended pitch counts per outing is one of the strongest predictors of arm injury
- Pitching more than 8 months out of the year significantly elevates risk
- Total annual pitches thrown is a stronger predictor of injury than any single-game workload
- Higher pitch velocity is also associated with increased elbow valgus torque and shoulder distraction force, meaning harder throwers may face additional risk

2. Mechanics & Technique
- Poor or fatigued mechanics place abnormal stress on structures that aren’t designed to compensate. Pitch velocity is the single most influential variable on both elbow valgus torque and shoulder distraction force, but several mechanical factors also significantly influence arm stress.
- Decreased hip-shoulder separation reduces the kinetic chain contribution to the throw, shifting load onto the arm
- Altered arm position during the cocking phase increases UCL stress
- Early trunk rotation, increased elbow flexion at ball release, and altered knee flexion at ball release have all been associated with increased shoulder and elbow torques
- Mechanical breakdown under fatigue is common and often goes unaddressed
- Don’t forget to check out our page on Throwing Mechanics

3. Physical Deficits
- Underlying physical limitations, many of which are silent until an injury occurs, are a significant and underappreciated risk factor. The American College of Sports Medicine identifies several physiological deficits as key contributors to the “disabled throwing shoulder,” including posterior rotator cuff weakness, altered shoulder rotation, scapular muscle weakness, and kinetic chain changes in core strength or flexibility.
- Glenohumeral internal rotation deficit (GIRD, a loss of internal rotation caused by posterior capsular contracture from repetitive throwing) is associated with shoulder injury in overhead athletes and has been linked to rotator cuff atrophy, weakness, and altered throwing biomechanics
- Scapular dyskinesis (altered scapular position or motion) has been associated with a 43% increased risk of developing shoulder pain in asymptomatic athletes, though a separate meta-analysis found it was not a statistically significant isolated risk factor for shoulder injury
- Core and hip weakness reduces the body’s ability to generate and transfer force efficiently, increasing arm load. Loss of hip internal rotation is specifically identified as a contributing factor

4. Age & Skeletal Maturity
- Youth athletes are not small adults. Growth plates represent vulnerable points that don’t exist in mature skeletons.
- Skeletally immature athletes are at disproportionate risk for physeal injuries (“Little Leaguer’s elbow” and “Little Leaguer’s shoulder”)
- Growth spurts can temporarily alter flexibility and coordination, increasing mechanical vulnerability
- Position changes (like moving from SS to P) during high-growth periods carry additional risk
5. Fatigue
- Fatigue is both a risk factor and a warning sign, and one of the most underreported in youth athletes. Research has demonstrated that as pitchers fatigue, medial elbow torque increases even as pitch velocity decreases, suggesting a dissociation between perceived effort and actual joint loading.
- Arm fatigue alters mechanics within a single outing, often before pitch count limits are reached
- Athletes (especially younger ones) frequently underreport fatigue due to social and competitive pressure
- Pitching while fatigued is one of the most consistently cited modifiable risk factors in the literature
- Arm fatigue has been identified as an independent risk factor for throwing arm injuries in adolescent baseball players

6. Early Specialization & Playing on Multiple Teams
- Early sport specialization and participation on multiple teams simultaneously have emerged as significant concerns, particularly at the youth level. A meta-analysis found that highly specialized athletes had an 81% increased risk of overuse injury compared with athletes with low specialization (RR 1.81, 95% CI 1.26–2.60). A separate meta-analysis found sport specializers had a 37% higher overall injury risk than sport samplers (RR 1.37, 95% CI 1.19–1.57).
- Playing on more than one team at a time removes meaningful rest periods and makes workload tracking nearly impossible
- Year-round single-sport training (more than 8 months per year) is associated with increased overuse injury rates
- Training more hours per week than the athlete’s age is associated with increased injury risk
- Playing for multiple teams has been identified as an independent risk factor for throwing arm injuries in adolescent baseball players
- Competitive and financial pressures on families often work against appropriate rest; awareness is the first line of defense

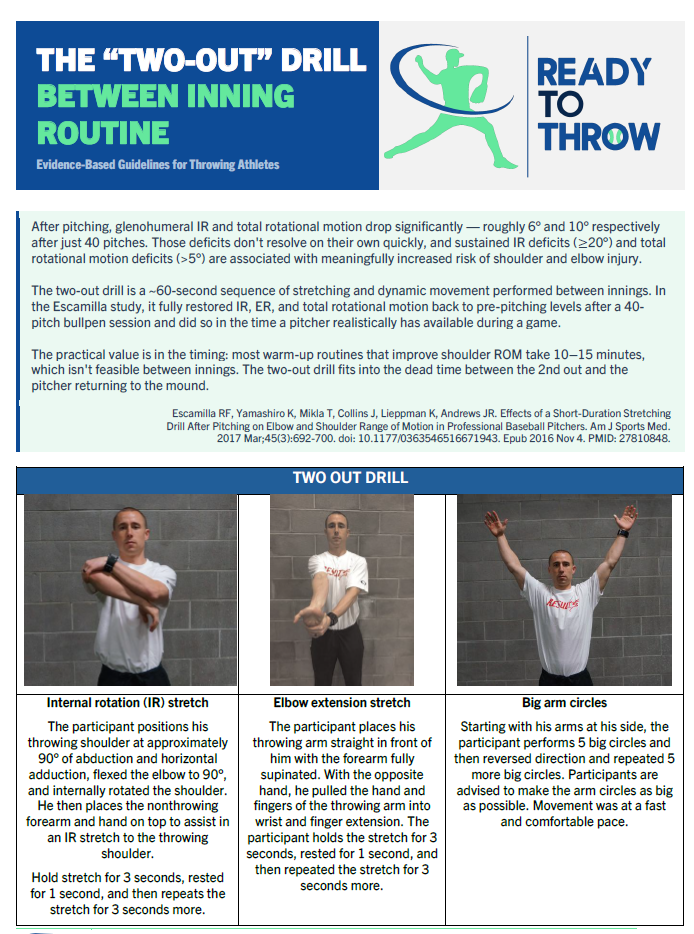
Make a Difference WHILE You Throw
The TWO OUT DRILL has been extensively researched by Escamilla et al. It integrates arm care directly into your throwing routine, so protecting your arm doesn’t require extra time. It just requires better intention behind every rep.
Escamilla RF, Yamashiro K, Mikla T, Collins J, Lieppman K, Andrews JR. Effects of a Short Duration Stretching Drill After Pitching on Elbow and Shoulder Range of Motion in Professional Baseball Pitchers. Am J Sports Med. 2017 Mar;45(3):692-700. doi: 10.1177/0363546516671943. Epub 2016 Nov 4. PMID: 27810848.
Prevention Strategies
Injury prevention looks a little different depending on your role.
Athletes

You are the most important variable in your own injury prevention. No coach, parent, or clinician can fully protect you if you aren’t paying attention to what your body is telling you.
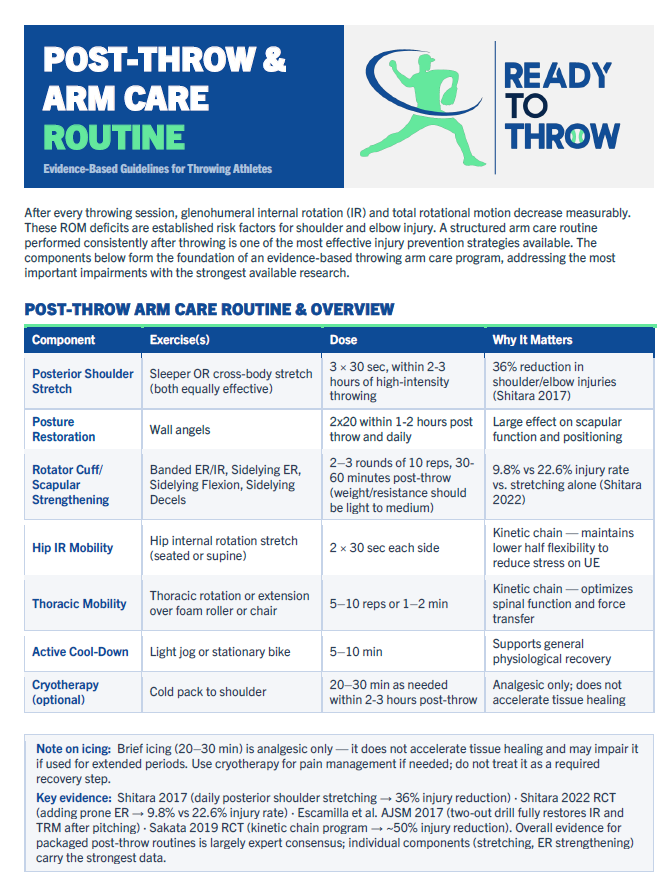
- Learn the difference between normal post-throwing soreness and pain that warrants stopping: soreness that fades within 24–48 hours after rest is generally expected; pain during throwing, sharp pain, or soreness that persists or worsens is not
- Never throw through pain. Communicate early, to your coach, your parents, and your athletic trainer, before a minor issue becomes a major one
- Invest in your arm care routine: a consistent pre- and post-throwing routine (band work, stretching, soft tissue work) is one of the most protective habits you can build
- Prioritize rest. Your arm recovers during rest, not during throwing. Protecting your off days is part of training
- Be honest about fatigue. Throwing while tired changes your mechanics in ways that increase injury risk, and no game is worth a season-ending injury
Coaches

Your decisions about pitch counts, rest, workload distribution, and how you respond to an athlete reporting discomfort have a direct impact on injury rates. The research is clear that coaching behavior is one of the most modifiable risk factors in the environment.
- Follow established pitch count and rest guidelines (see Section 05) and treat them as floors, not ceilings; guidelines don’t account for an athlete’s cumulative fatigue, mechanics, or physical condition on a given day
- Learn to recognize mechanical fatigue: dropping elbow, loss of hip-shoulder separation, decreased velocity, and altered release point are signs an athlete is breaking down
- Create an environment where athletes feel safe reporting arm discomfort without fear of losing playing time. Athletes who hide pain are athletes who get hurt
- Monitor multi-team participation among your athletes; if a player is pitching for another team, you may be significantly underestimating their total workload
- When in doubt, rest. The cost of an unnecessary rest day is minimal. The cost of ignoring early warning signs is not
Parents

Parents are often the most important, and often least empowered, people in this conversation. You see your athlete across contexts that coaches don’t. Research suggests that up to 83% of caregivers are not aware of sport-specific injury prevention guidelines.
- Know the pitch count and rest guidelines for your child’s age group, and don’t assume someone else is tracking them, especially in multi-team situations
- Watch for warning signs: your child favoring their arm, rubbing their elbow or shoulder, decreased velocity, or reluctance to throw are all worth paying attention to
- Normalize rest and honest communication in your household: athletes who feel pressure to perform through pain often do so to meet perceived expectations from parents as much as coaches
- Multi-team and year-round play is one of the most significant risk factors for youth throwing injuries. It’s worth having an honest conversation about workload, even when it’s a difficult one
- Trust your instincts. If something looks or sounds wrong, advocate for evaluation. Early intervention is almost always better than waiting
Clinicians

This section assumes familiarity with overhead athlete assessment and throwing biomechanics. The following reflects general consensus from the literature rather than clinical protocol.
- Incorporate throwing-specific screening into routine evaluations: shoulder ROM (total arc, GIRD), scapular mechanics, hip mobility, and rotator cuff strength are the most consistently implicated physical deficits in the literature
- Obtain a thorough workload history, including pitch counts, teams, months of play, and recent changes in volume or intensity
- Communicate proactively with coaches and athletic trainers when appropriate; the athlete exists within a system, and clinical recommendations without environmental context often go unimplemented
- Return-to-throw progressions should be individualized, not calendar-based – Be familiar with the Pitch Smart and USA Baseball guidelines so you can speak to them directly with families and coaching staff
Additional references:
- Smith S. The Effect of Stride Length on Pitched Ball Velocity. Spring 2017 Baseball Research Journal
- Ramsey DK, Crotin RL, White S. Effect of stride length on overarm throwing delivery: A linear momentum response. Hum Mov Sci. 2014 Dec;38:185-96. doi: 10.1016/j.humov.2014.08.012. Epub 2014 Nov 9. PMID: 25457417.
- Rod Whiteley. (2007) Baseball Throwing Mechanics as They Relate to Pathology and Performance – A Review. Journal of Sports Science and Medicine (06), 1 – 20.
- Manzi JE, Yu JS, Sudah SY, et al. A Systematic Review of Lower-Body Kinematic and Strength Factors Associated With Pitch Velocity in Adult Baseball Pitchers. Journal of Sport Rehabilitation. 2023;32(4):440-448. doi:10.1123/jsr.2022-0059
- Van Trigt B, Schallig W, Van der Graaff E, Hoozemans MJM, Veeger D. Knee Angle and Stride Length in Association with Ball Speed in Youth Baseball Pitchers. Sports. 2018; 6(2):51. https://doi.org/10.3390/sports6020051
- Douoguih WA, Dolce DL, Lincoln AE. Early Cocking Phase Mechanics and Upper Extremity Surgery Risk in Starting Professional Baseball Pitchers. Orthopaedic Journal of Sports Medicine. 2015;3(4). doi:10.1177/2325967115581594
- Diffendaffer AZ, Bagwell MS, Fleisig GS, Yanagita Y, Stewart M, Cain EL Jr, Dugas JR, Wilk KE. The Clinician’s Guide to Baseball Pitching Biomechanics. Sports Health. 2023 Mar-Apr;15(2):274-281. doi: 10.1177/19417381221078537. Epub 2022 Apr 23. PMID: 35465789; PMCID: PMC9950989.
MORE INFORMATION COMING SOON!
In need of some help? Looking for a professional throwing mechanics analysis?

Let our experts handle it.
Our team is here to help you perfect your form, prevent injuries, and maximize your performance. Whether you’re a seasoned athlete or just starting, a professional throwing mechanics analysis can provide the insights you need to excel.
Click the button to learn more and fill out our request form and get started on your journey to better mechanics and enhanced performance today!